
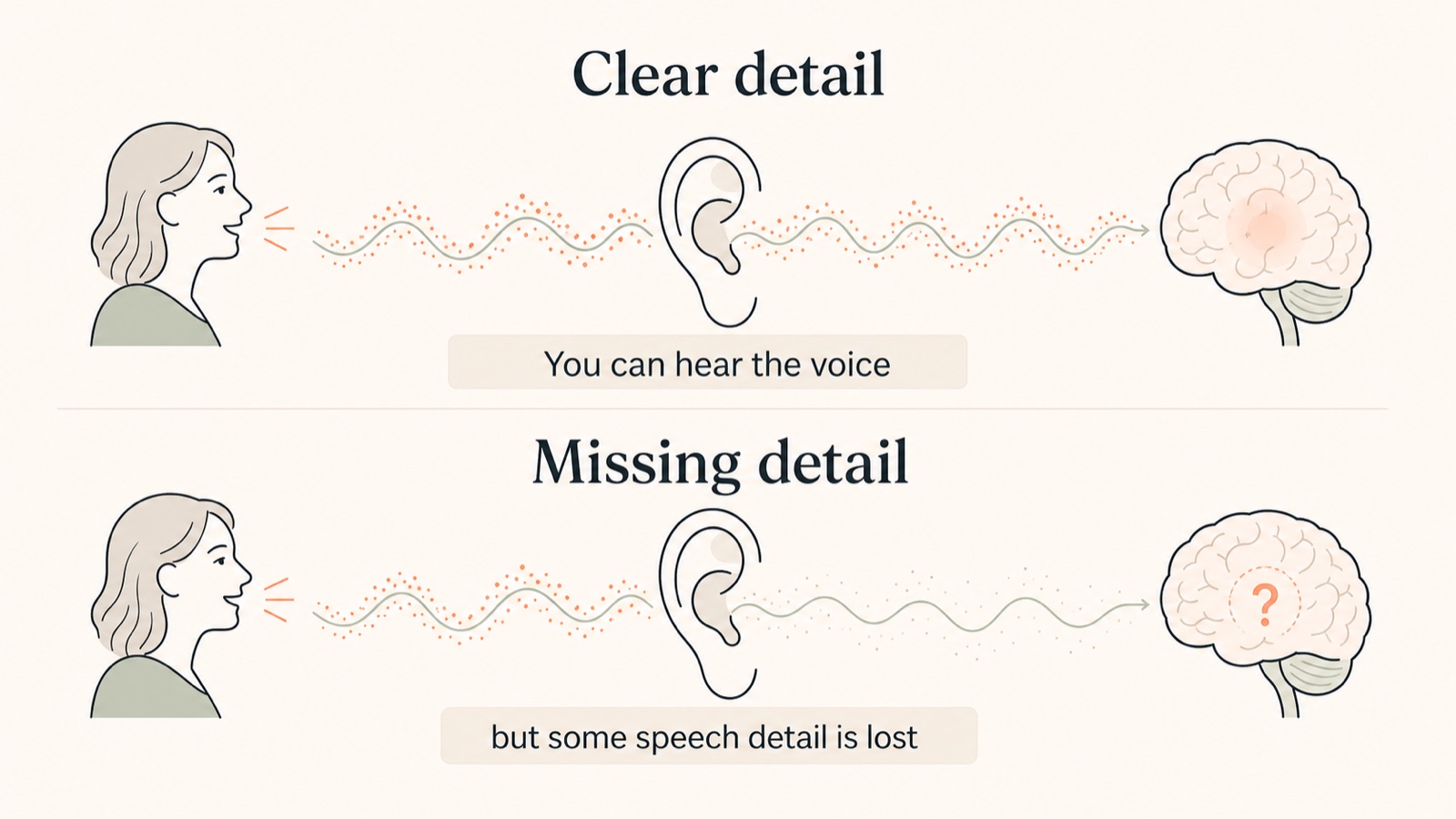
Hearing loss does not always make everything quieter. For many people, it first shows up as lost clarity. You can hear a voice, but not catch every word.
Patients often describe it as inconsistent. You may hear well at home, then lose the thread in a restaurant. You may hear a voice from another room, but not the exact words. You may hear your partner talking, but feel as though they have started to mumble.
Below, we explain what hearing loss is, why speech can become unclear, what signs to look for, when to seek urgent medical help, and what a thorough hearing assessment should tell you.
Clinically reviewed by Adam Bostock, Audiologist. Last reviewed 12 May 2026.
When hearing loss needs urgent help
If your hearing has suddenly changed in one or both ears, or has become noticeably worse over a few days or weeks, do not wait for a routine hearing appointment. Contact NHS 111 or ask for an urgent GP appointment.
Seek urgent advice sooner if the change is one-sided, or if you also have dizziness, severe tinnitus, ear pain, discharge, facial weakness or any other symptoms that feel unusual for you.
What hearing loss often feels like
Hearing loss is not always obvious at first. Many people compensate for years without realising it. They lip-read a little more. They pick calmer tables. They avoid group conversations. They blame the room, the speaker, the television, or their own concentration.
The earliest signs are often small and practical:
- speech sounds less clear, especially in background noise
- people seem to mumble
- you hear better when you can see someone’s face
- you ask people to repeat themselves, particularly in groups
- the television or phone volume creeps up
- you avoid busy places because listening feels tiring
- family members notice before you do
If those examples feel familiar, try our hearing loss simulator. It is not a diagnostic test, but it shows why someone can hear a voice and still miss parts of the words.

Why hearing loss affects speech clarity
Before sound becomes something you understand, it has to pass through the outer ear, the eardrum, the middle ear bones, the inner ear and the hearing nerve. Only then can the brain interpret it.
Many adult hearing losses start in the inner ear. Inside the cochlea are delicate sensory cells that help convert sound vibration into electrical signals. When those cells are damaged by age, noise, certain medical conditions or other causes, the brain receives less detail.
Speech relies on fine detail. Vowels carry volume and rhythm. Consonants carry precision. Sounds like “s”, “f”, “th”, “t” and “k” are easy to lose when high-frequency hearing drops. The voice may still be audible, but the edges of the words become less distinct.
What we look for in clinic
The tone test is only part of it. We also look at whether speech remains clear, how you manage background noise, and whether the ear itself needs attention.
Two people can have similar results on paper and still need different advice.
The main types of hearing loss
Clinically, hearing loss is described by where the problem sits in the hearing system.
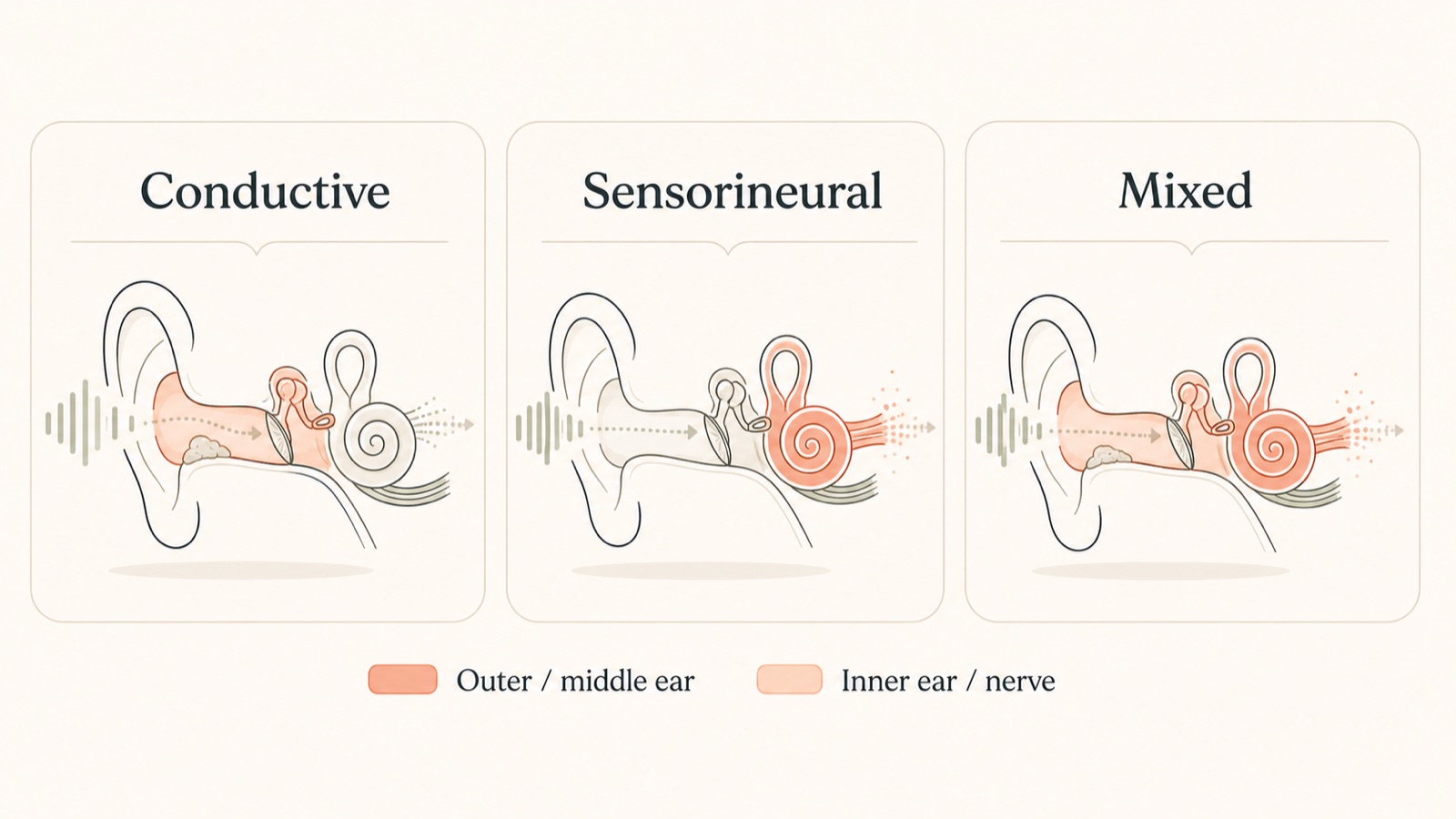
The name tells us where the problem sits in the hearing system.
Conductive hearing loss
Sound is blocked or reduced before it reaches the inner ear. The issue is usually in the outer or middle ear, such as wax, infection, fluid behind the eardrum or a perforated eardrum. It often makes sound softer or muffled, and some causes are temporary and treatable.
Sensorineural hearing loss
The inner ear, the hearing nerve, or both are not passing on sound detail as clearly as they should. This is the most common type of permanent adult hearing loss and is often linked to age, noise exposure or more than one cause.
Mixed hearing loss
Both are happening at the same time. Someone may have long-term inner-ear hearing loss and also have wax or a middle-ear issue making things worse. Ear health checks help separate those layers before deciding what support is needed.
Common causes of hearing loss
The same symptom can come from different parts of the ear. A hearing assessment measures hearing levels, but it also checks whether the pattern looks like wax, middle-ear involvement, inner-ear damage, or something that needs medical referral.
| What you notice | Possible explanation | Best next step |
|---|---|---|
| Gradual change in both ears over years | Often age-related hearing loss, noise-related hearing loss, or both | Book a Complete Hearing Assessment if it is affecting daily life |
| Blocked feeling, usually in one ear | Ear wax can be involved, but it is not the only possibility | Have your ears checked before assuming it is wax |
| Ear pain, discharge, fever or itching | Possible ear infection or inflammation | Speak to your GP or pharmacist, depending on symptoms |
| Sudden loss or rapid worsening | May need urgent medical assessment | Contact NHS 111 or ask for an urgent GP appointment |
| Hearing difficulty with tinnitus | Often linked, but the cause needs context | Arrange assessment, and seek medical advice if sudden or one-sided |
Ear wax is a common and often treatable cause of muffled hearing. But if hearing does not return after wax removal, or if your symptoms do not fit a simple blocked-ear picture, the next step should be a broader hearing assessment. You can read more about our ear wax removal service and what we check if wax is not the answer.
Why background noise is often the first problem
Many people with early hearing loss manage well in calm, one-to-one conversation. The difficulty shows up when sound becomes complicated.
In a restaurant, the voice you want is competing with music, cutlery, chairs, other voices and room echo. Your brain has to separate the signal from the noise. If the signal arriving from the ears is already reduced or blurred, that separation becomes much harder.
You might hear better at home than in a cafe, better with one person than in a group, and better when you can see someone’s face. Listening can also feel tiring, because the brain is filling in more gaps.
We explain this in more detail in our guide to why background noise makes hearing harder.
What happens if hearing loss is left alone?
What happens next depends on the cause. Some hearing losses need medical treatment, some need monitoring, and some are best helped with hearing aids. Ignoring the problem usually means conversations become harder work.
The practical impact is often bigger than the hearing result suggests. Conversations take more effort. People withdraw from noisy places. Partners start repeating themselves. Family meals become harder to follow. Work meetings become more draining. Confidence changes before the person has even called it hearing loss.
A careful note on brain health
Researchers now study hearing loss as part of brain health. The evidence does not show that hearing loss directly causes dementia, or that hearing aids prevent dementia. It does show a consistent association. A 2024 systematic review and meta-analysis found adult-onset hearing loss was associated with higher later risk of cognitive decline, mild cognitive impairment and dementia. A large 2024 Danish cohort study also found higher dementia risk in people with hearing loss, particularly where hearing aids were not being used. A 2025 US cohort study estimated that objectively measured hearing loss accounted for a substantial proportion of dementia risk at population level.
Clinically, the concern is plausible without needing to overstate it. Poor hearing can mean more listening effort, fewer conversations, more withdrawal from noisy places and less easy social contact. Those changes may contribute to cognitive load and isolation, both of which are relevant to wider health. So we should not use dementia fear to sell hearing aids. But we also should not treat hearing as separate from the rest of health.
An early assessment gives you a baseline, shows whether there is anything medically obvious to address, and helps you decide whether to monitor, use communication strategies, start with a screening appointment, or consider hearing technology.
What a good hearing assessment should tell you
A good assessment should not leave you staring at a graph. It should explain what the results mean when you are talking to people, listening in noise, or trying to follow a busy room.
At Alto, a Complete Hearing Assessment looks at ear health, hearing levels, speech clarity, speech-in-noise ability and the situations where hearing is becoming difficult. We use the results to explain what is happening in the places where hearing has to work hardest: kitchens, restaurants, cars, meetings, shops and family gatherings.

A thorough assessment should help answer:
- Is there hearing loss, and is it in one ear or both?
- Does the pattern look conductive, sensorineural or mixed?
- Is ear wax, middle-ear pressure or infection likely to be involved?
- How well do you understand speech in background noise?
- Are hearing aids likely to help, or is monitoring more appropriate?
- If hearing aids are suitable, what level of support and fitting quality do you need?
What can help hearing loss?
What helps depends on the cause.
If hearing is reduced because of wax, infection or another outer or middle-ear issue, medical treatment or wax removal may improve it. If hearing loss is permanent, the work is to improve access to speech, reduce listening effort and make everyday communication easier.
Options can include:
- communication changes, such as facing the person and reducing background noise
- hearing protection to prevent further noise damage
- hearing aids matched to your hearing, lifestyle and listening needs
- hearing-aid fitting and verification, so the devices are matched accurately to your hearing
- Real Ear Measurements, where appropriate, to check what the hearing aids are doing in your ears
- ongoing hearing-aid aftercare and adjustment as your brain adapts
Hearing aids are only one part of treatment. The assessment, explanation, fitting, follow-up and long-term support all affect how well someone gets on.
If you are helping someone else with hearing loss
Family often notice hearing loss before the person experiencing it is ready to talk about it. The conversation can be delicate, so keep the focus on specific situations rather than blame.
Try using specific, non-judgemental examples. “You seemed tired after lunch because the restaurant was noisy” is usually better than “you never listen”. If you are supporting a parent or partner, our guide to helping a parent with hearing loss may help.

What to do next
If you are unsure whether hearing loss is present, SoundCheck is a free hearing health check that can show whether anything needs attention.
If hearing is affecting conversations, confidence, work, family life or social situations, book a Complete Hearing Assessment. Your audiologist can examine the ears, measure the hearing in detail and explain whether to monitor, treat, or consider hearing technology.
Hearing loss FAQs
Can hearing loss come and go?
Yes. Wax, middle-ear pressure, infection and Eustachian tube problems can fluctuate. Sensorineural hearing loss is usually more permanent. If hearing changes suddenly, rapidly or in one ear, seek medical advice rather than guessing the cause.
Does hearing loss always mean I need hearing aids?
No. Wax, infection or middle-ear problems may need a different route. Some people monitor their hearing for a while. Others do well with hearing aids.
Why can I hear people talking but not understand the words?
Often because the high-frequency consonants are missing or blurred. You may detect the voice, but lose the small speech cues that separate one word from another.
Is background noise difficulty an early sign of hearing loss?
It can be. Restaurants, family gatherings and group conversations often become difficult before one-to-one conversation does. Speech-in-noise testing can measure this more realistically than a simple tone check alone.
What should I do if my hearing suddenly changes?
Contact NHS 111 or ask for an urgent GP appointment. Sudden or rapidly worsening hearing loss should not wait for a routine private hearing appointment, especially if it is one-sided or comes with dizziness, tinnitus, pain, discharge or other unusual symptoms.
Sources
Source checked May 2026: NHS hearing loss guidance, NICE hearing loss in adults guidance, RNID signs of hearing loss, RNID types and causes of hearing loss, WHO safe listening guidance, American Academy of Audiology listening fatigue information, a 2024 Ageing Research Reviews systematic review and meta-analysis, a 2024 JAMA Otolaryngology Danish cohort study, and a 2025 JAMA Otolaryngology cohort study on dementia risk attributable to hearing loss.